Coronary Arteries
The Coronary Arteries Supply Nutrients and Oxygen to the Myocardium
The heart is the pump that supplies blood, oxygen, and other nutrients to the entire body. However, the heart itself is an organ that requires its own blood supply to maintain proper function. The coronary arteries supply blood, oxygen, and nutrients to the heart muscle and the conduction system. Because the LV muscle mass exceeds that of the RV and has a greater blood and O2 requirement, the coronaries supply more blood to the LV. Coronary veins remove waste and CO2 laden blood from the myocardium, dumping blood back to the coronary sinus.
|
|
The right and left coronary arteries are the two principal coronary arteries. They originate at the base of the aorta, commonly known as the aortic root. Blood flows through ever-smaller ramifications that branch out over the surface of the heart, and then within the muscle, into a fine capillary network that reaches individual myocardial fibers. It is the distribution of adequate and inadequate coronary arterial blood supply that is imaged by radioactive myocardial perfusion imaging agents.
The Right Coronary Artery descends along the inferior (bottom) border of the right atrium. It then courses to the right, in the atrioventricular groove between the right atrium and the right ventricle, and around the lateral wall of the heart to the posterior surface of the right ventricle. It then sends descending branches (posterior descending rami) down the ventricular wall.
The RCA supplies the right ventricular wall, the posterior part of the interventricular septum, and most of the inferior wall of the left ventricle. In about 50% of people, the right coronary artery also supplies the area of the right atrium near the orifice of the superior vena cava where the sinoatrial node, the pacemaker of the heart, is located. In other people, this area is supplied by a branch of the left circumflex artery. In 90% of people, the right coronary artery also supplies the area of the atrioventricular node just beneath the surface of the septum dividing the right atrium from the right ventricle.
The Left Coronary Artery arises from the aortic root as a single short main left coronary artery, the left mainstem. The left mainstem bifurcates to form the:
- Left anterior descending artery. The left anterior descending artery (LAD) courses down between the two ventricles anteriorly in the interventricular groove and supplies the interventricular
septum, the apex, and the anterior wall of the left ventricle. - Left circumflex. The left circumflex (LCx) travels as its name implies: circum, meaning around, and flex, meaning to bend. That is, the LCx passes around the groove between the left atrium and the left ventricle where it bends and courses along the lateral and posterior portions of the left ventricle. In some people, the LCx is responsible for supplying blood to the sinoatrial node (SA).
|
|
Surface Vessels and End Arteries
The ramifications of the coronary arteries run along the surface and branch into the wall of the heart. Similar to arteries elsewhere in the body, the coronary arteries branch into small arteries and arterioles. These vessels terminate in end arteries that supply the myocardial tissue with blood.
In the capillaries, oxygen- and nutrient-rich blood is delivered to the myocardium while carbon dioxide and other waste products are removed. Blood then flows into small venules and veins leading to larger venous channels. Virtually all the blood from the left coronary artery drains through the coronary veins, through the coronary sinus, and into the right atrium. The blood from the right coronary artery drains mainly into the anterior cardiac veins and into the right atrium.
Supply and Demand
The blood flow in the coronary arteries resembles arterial flow to other regions of the body in that it is dependent on the blood pressure and the vascular resistance. The coronaries must be able to respond to the varying requirements of the heart muscle, especially that of the ventricles. Because the muscle mass of the left ventricle exceeds that of the right ventricle, the coronary arteries need to supply more blood and oxygen to the left ventricle than to the right. A unique feature of the coronary circulation is that the arteries are compressed by the contracting myocardium during systole, thereby increasing the resistance to blood flow. The blood flow through coronary circulation is restored during diastole.
In the normal resting heart, unlike other organs, almost all the oxygen is extracted from the blood during its passage through the arterioles and the capillary beds. Therefore, when faced with increased oxygen demand during exercise or stress, the heart is dependent upon the coronary arteries to increase their diameter through dilatation. Exercise or stress increases heart rate, blood pressure, and contractility of the ventricle, all of which demands the coronary arteries to provide enough oxygen to the working myocardium. In the healthy heart, the coronary arteries can meet this increased demand by dilating and increasing coronary blood flow, thus providing more oxygen to the myocardium.
When coronary artery disease decreases the elasticity or obstructs flow through a coronary artery, the blood supply to the area served by the artery is threatened. This inadequate blood supply deprives the muscle tissue of sufficient oxygen and nutrients to function normally, a condition called ischemia. During exercise, if the demand for blood outstrips the supply, the ventricular muscle is deprived of sufficient oxygen to continue the work of pumping-and the muscle signals its distress with angina.
SHORT AXIS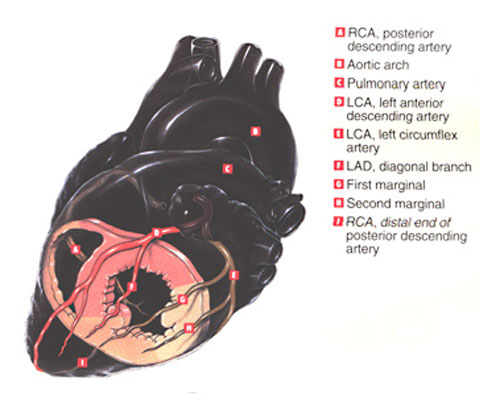 |
HORIZONTAL LONG AXIS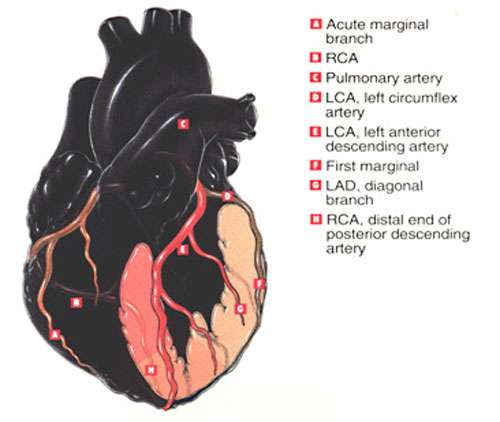 |
VERTICAL LONG AXIS |
Collateral Circulation
The coronary arteries are located in the epicardial surface of the heart, while smaller branches of these arteries are embedded into the myocardial and subendocardial surfaces of the heart muscle. These vessels are end vessels that communicate freely to supply myocardial tissue with blood. There are many small anastomoses between the coronary arteries, but sometimes these are of no functional importance. However, when a large area of the heart is deprived of blood, these anastomoses enlarge and then provide a collateral blood supply to the affected muscle. Exercise helps to enhance circulation to compromised myocardium.
The growth of atherosclerotic plaques into lesions large enough to obstruct blood flow is a gradual process. If an artery becomes completely occluded by plaque, it will often form bridging collaterals to healthy arteries. This keeps local myocardium viable despite the vessel occlusion. Over time, these smaller vessels dilate and are able to increase blood supply to the ischemic area.
Myocardial Oxygen and Nutrient requirements
The human heart requires more energy than any other organ in the body.
The myocardium functions almost solely on aerobic metabolic pathways,
and a deprivation of oxygen for more than 2 minutes results in total
cessation of myocardial activity. Myocardial hypoxia produces prompt
coronary vasodilation.
Resting myocardium receives less than 5% of the cardiac output. With
exercise, oxygen consumption of the heart may increase three- to
five-fold. Cardiac muscle extracts 70% of the oxygen in every
milliliter of blood delivered to it.
The coronary arteries bring nutrients and oxygen to the heart to sustain
its activity. About 60% of the energy for heart activity is derived
from the metabolism of fatty acids; 35% comes from the metabolism of
carbohydrates; 5% comes from the metabolism of amino acids. Inorganic
salts are extremely important in the regulation of the beat and
depolarization of heart muscle.
Low blood sodium levels
(hyponatremia) interferes with the depolarization of the heart muscle, and the heartbeat ceases.
Increase or decrease in blood potassium levels
(hyper- and hypokalemia) cause difficult depolarization and repolarization, respectively.
Increased blood calcium level
(hypercalcemia) results in rapid uncoordinated contraction or fibrillation of the cardiac muscle.
Low blood magnesium levels lengthen a beat, and high blood magnesium levels cause cardiac arrest.
CORONARY FLOW
As in the rest of the body, arterial flow in the coronary arteries is dependent on the blood pressure and vascular resistance. Because of its greater muscle mass, the LV needs a greater supply of oxygen and blood than the RV. The arteries are compressed by the contracting myocardium during systole, which increases resistance to blood flow. Flow is restored during diastole.
Exercise or stress causes the heart rate and blood pressure to increase as the contractility of the left ventricle increases to meet the oxygen demand of the working muscle.
In the healthy heart, the coronary arteries can meet increased demand by dilating and increasing coronary blood flow, delivering more oxygen. When coronary artery disease decreases the elasticity or obstructs flow through the coronary artery, the blood supply served by that vessel is threatened. An inadequate supply of oxygen causes ischemia, which may lead to angina.
Consequences of impaired blood flow to the conduction system are variable:
Blockage of posterior branch of the RCA will typically cause transient changes in the conduction system through the AV node.
Impairment of circulation of the LAD usually results in a large myocardial infarction that may damage the bundle branches
1) tissue death in bundle branches leads to permanent conduction delay
2) a heart block occurring at this level requires a permanent pacemaker